This SleepSomatics blog article is part three of a four part series on sleep quality, sleep disorders, sleep & weight loss, and in-lab sleep study testing.
Part One: What is the Sleep Architecture
Part Two: What is Restorative Sleep
Part Three: What Causes Deficient Restorative Sleep
Part Four: Restorative Sleep and Weight Loss

What Causes Deficient Restorative Sleep
In Part One: What is the Sleep Architecture, we reviewed how one-third of life is spent sleeping, and yet, given the necessity for quality sleep in overall health and well-being, one in three Americans are deprived of sleep and 9 out of 10 sleep disorder sufferers go undiagnosed and untreated. We learned that the two important stages of deep, restorative sleep include:
- Stage N3 delta slow-wave sleep is physiologically restorative and produces, releases, or balances important hormones, blood sugar, metabolism, and energy.
- Stage REM sleep is cognitively restorative and assists in the consolidation of memories and stabilizing of mood and temperament.
In Part Two: What is Restorative Sleep, we discussed how sleep is a dynamic state of alternating deep and light sleep cycles known as the sleep stages or sleep architecture. The deep sleep stages delta and REM are considered restorative, where neurological, physiological, and hormonal restoration and repair occurs. Restorative sleep deficiencies result in:
- Automobile accidents
- Cognitive dysfunction, difficulty remembering things, difficulty focusing
- Male sexual dysfunction including belly fat, weight gain, muscle loss, low testosterone, low libido, impotence
- Poor energy and fatigue
- Psychiatric or mood disorders including depression, mood swings, anxiety, or Attention Deficit Hyperactivity Disorder (ADHD)
- Reduced quality of life and satisfaction
- Weight gain or difficulty losing existing weight and obesity
RELATED: ORDER YOUR HOME SLEEP APNEA TEST & CONSULTATION TODAY
Sleep Architecture Overview
Adults will mostly progress through sleep architecture cycles every two hours in a predictable model, with increased Stage N3 delta sleep when first going to sleep and increasing Stage REM sleep when approaching the end of sleep. Restorative sleep should account for 50% of one's sleep, divided evenly between Stage N3 delta and Stage REM sleep.
Stage N1 -> Stage N2 -> Stage N3 -> Stage N2 -> Stage REM -> Repeat
When a patient contacts an accredited Austin sleep lab like SleepSomatics for sleep testing, their symptoms often indicate restorative sleep deficiency. Often, the patient has already undergone blood work testing to explain their fatigue, weight, mood, or libido problems, including thyroid, testosterone, human growth hormone, estrogen, iron, Vitamin D, Vitamin B-12, magnesium, etc. Or, the patient has tried anti-depressant medications, vitamin supplements, and hormone replacement therapy. Yet their fatigue symptoms remain. So when the patient is referred to a sleep lab Austin SleepSomatics for an in-lab sleep study, they have exhausted all other options for finding both cause and treatment for their poor performance and reduced quality of life.
What Happens During a Sleep Study
During an attended polysomnogram (in-lab sleep study), the sleep architecture and restorative sleep indices are quantified. Brain waves are measured and recorded along with corresponding or concurrent physiological events or episodes. An in-lab sleep study visualizes and determines the brain waves emitted on a second-to-second basis, allowing a sleep medicine specialist like SleepSomatics to precisely quantify:
- When a person is truly neurologically awake or asleep
- What type of sleep they are experiencing (sleep stages)
- How often they are waking up
- Why they are waking up
Related: Drowsy Driving Responsible for 1 in 5 Automobile Accidents
Sleep Architecture and the Human Brain
The human brain wants to progress through the sleep architecture and capture the necessary restorative sleep. Adolescents, for example, experience much greater percentages of delta sleep as their bodies physically grow and mature, and by the time we reach our 70's and 80's, we have far lower indices of delta sleep as the body's requirements for growth diminish. In the vast majority of patients with restorative sleep deficiency, the reason for the deficiency is because something is disrupting that sleep architecture cycling. Absent external forces (like a spouse or bed partner with his or her own undiagnosed and untreated sleep disorder like snoring, sleep apnea, or restless leg syndrome), there are three categories for sleep architecture disruptions that reduce or prevent restorative sleep:
- Arousals and Awakenings
- Medication
- Lifestyle
Arousals and Awakenings
Arousals are periods lasting 3-14 seconds where the brain wave frequencies shift or change from a neurological state of sleep to a neurological state of wakefulness. Arousals can occur a couple times per hour to several hundred times over the course of a night, and most often patients are completely unaware of arousals.
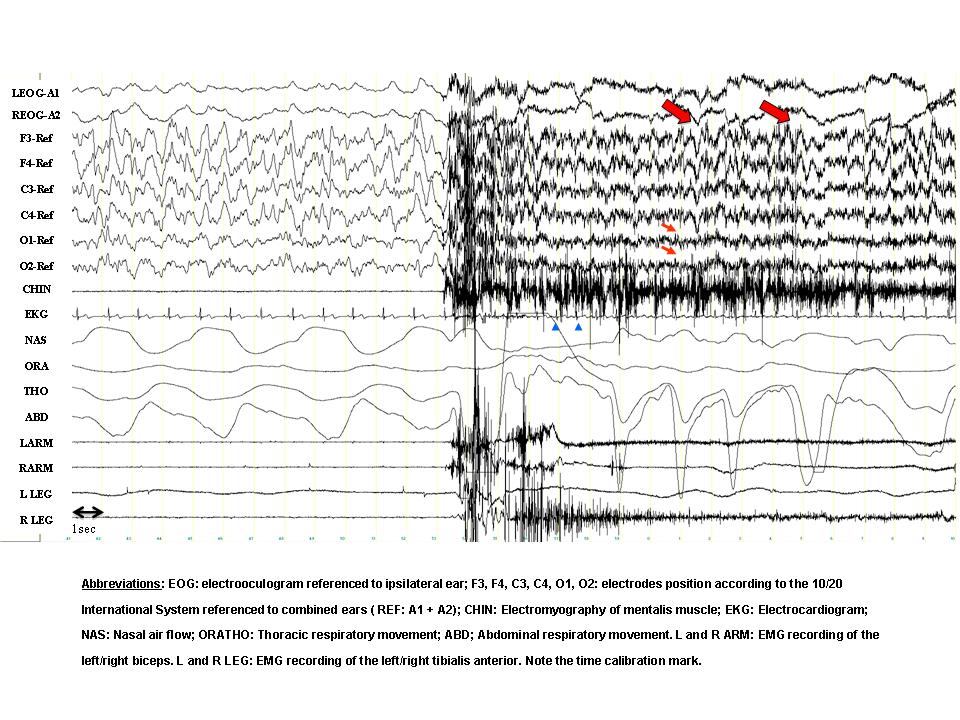
In this example, the first half of the window shows normal Stage N3 delta slow-wave sleep. At about half-way through, there is a sudden change in the EEG brain wave activity, shifting the patient from neurological sleep to a state of wakefulness.
Awakenings are periods lasting 30 seconds or more where a person completely awakens, often opening their eyes as they shift around in bed, change sleep positions. A person can fall back asleep quickly after an awakening, or they can remain awake for long periods of time. Awakenings, unlike arousals, are usually perceived by the patient. When a person is asked how often they wake up during the night, it is awakenings that they report (not arousals).
An in-lab sleep study from a Austin sleep lab like SleepSomatics can tell a patient how often they are waking up from arousals and awakenings and, more importantly, what is causing the arousals or awakenings. Quantifying and eliminating arousals with sleep testing is critical because sleep quantity doesn't matter if sleep quality is poor.
The two most common causes we at SleepSomatics see in our sleep lab Austin for patients with excess arousals or awakenings:
- Sleep-disordered breathing, including sleep apnea and snoring
- Periodic limb movement disorder or Restless Leg Syndrome
Sleep-Disordered Breathing, Sleep Apnea, Snoring, and Upper Airway Resistance Syndrome
Sleep-disordered breathing (sleep apnea) and snoring occur when there is a blockage or restriction in the airway. This restriction reduces oxygen saturation, increases heart rate and blood pressure, and causes the release of stress hormones. As the airway begins to collapse, the body sends signals to the brain to open the muscles through some kind of physical movement or action, which often is when a sleep apnea sufferer snorts, chokes, gasps, coughs, or moves their head in some way.
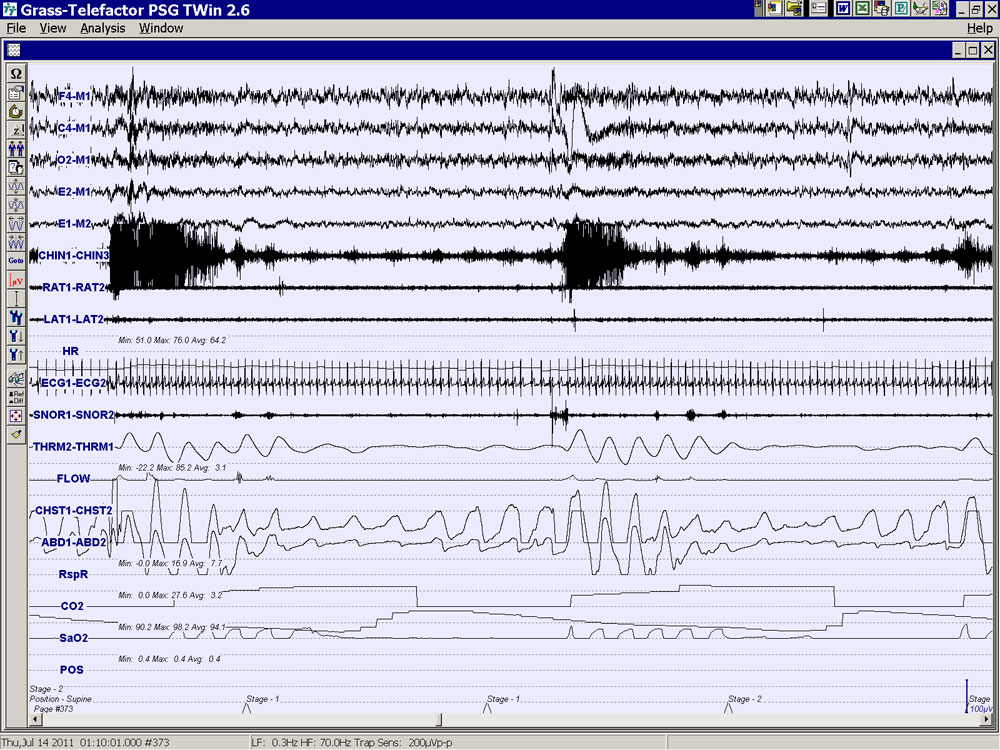
In this example, this patient is experiencing sleep apnea episodes of breathing pauses. The CO2 monitor shows increasing carbon dioxide as the SaO2 monitor shows plummeting oxygen desaturations and hypoxia. In the Chin and EEG brain wave activity we see the patient's brain is briefly waking the patient up with corresponding arousals in response to the sleep apnea. And yet, after each arousal and airway opening, the patient falls right back asleep, the sleep apnea resumes again, and another corresponding arousal occurs. This sleep apnea severity is likely responsible for significant sleep architecture disruption, paucity (or reduced) restorative sleep, daytime fatigue and sleepiness, reduced concentration at work or when driving, and many other significant health risks. The repeated loss of oxygen and increased carbon dioxide also stress the heart and increase hypertension, diabetes, heart attack, and stroke risk factors.
This physical action resolves the apneic episode, opening the airway and restoring oxygen, but this movement also produces an arousal, temporarily waking the patient and disrupting the normal sleep architecture. When Austin sleep lab SleepSomatics treats sleep apnea with CPAP therapy, we improve sleep architecture and restorative sleep by eliminating the associated arousals and snoring.

In this example, the patient is experiencing a sleep apnea episode as indicated in the flat line. Once the flat line suddenly resumes breathing with the opening of the airway, the EEG brain waves above indicate a sudden and temporary shift from neurological sleep to neurological wakefulness lasting only a few seconds. The patient then falls back asleep, not realizing that they just briefly awoke. This patient's sleep apnea severity likely wakes the patient from sleep hundreds of times per night, violently disrupting the sleep architecture and potentially reducing the patient's restorative sleep.
Portable at-home sleep testing (take-home sleep testing) measures and screens for sleep apnea and snoring. However, this form of limited channel unattended testing does not evaluate or quantify the sleep architecture, restorative sleep, arousals, or awakenings.
Restless Leg Syndrome and Periodic Limb Movements of Sleep
Periodic limb movements of sleep (periodic leg movements) and restless leg syndrome (restless limb syndrome) are two separate disorders that are idiopathic (meaning doctors are uncertain of the specific cause of each) but are nonetheless treated with similar medications. Periodic limb movements of sleep, as the name suggests, occur in regular rhythmic twitches during sleep, and sufferers and their bed partners are often unaware of the condition because it occurs during sleep and is quite subtle. However, periodic leg movements can produce arousals, thus fragmenting the sleep architecture and reducing restorative sleep. Restless leg syndrome is occurs when a patient is awake and is usually quite noticeable since the sufferer feels discomfort in their legs and moves them to alleviate the sensation, alerting both the patient and his or her bed partner.
Psychiatric Medication Effects on Sleep Architecture and Restorative Sleep
Alterations or changes to the sleep architecture are a common side-effect of many psychiatric medications. Anti-depressant medication usage is exploding in the United States. It therefore isn't uncommon to experience sleep disturbances as a result of antidepressant medication usage.
It must be stated here that you should never alter or adjust your prescription medication usage without direction from or supervision of the prescribing physician. Nor should a patient assume that because a medication is listed below that Stage N3 delta or Stage REM suppression or sleep disruption are guaranteed or confirmed effects.
The list below is only a sample of medications within those categories or medication groups, and it is the groups that are commonly associated with sleep architecture changes. Patients who take these medications and have sleep problems or related symptoms should consider asking their doctor to order an in-lab sleep study with sleep lab SleepSomatics to evaluate their sleep architecture and quantify their restorative sleep indices. Once an individual's sleep architecture is analyzed and quantified, then a sleep medicine specialist can consult with the prescribing physician on what (if any) adjustments are recommended.
Psychiatric prescription medications that can potentially reduce, delay, or worsen physiologically-restorative and hormone-balancing Stage N3 delta slow-wave sleep and/or reduce cognitively-restorative Stage REM sleep include:
- Benzodiazepines
- Alprazolam (Xanax)
- Clonazepam (Klonopin)
- Diazepam (Valium)
- Lorazepam (Ativan)
- Temazepam (Restoril)
- MAOI (monoamine oxidase inhibitor)
- Isocarboxazid (Marplan)
- Phenelzine (Nardil)
- Selegiline (Emsam)
- Tranylcypromine (Parnate)
- Selective SNRI (serotonin and norepinephrine reuptake inhibitor)
- Desvenlafaxine (Pristiq)
- Duloxetine (Cymbalta)
- Venlafaxine (Effexor)
- SSRI (selective serotonin reuptake inhibitors)
- Citalopram (Celexa)
- Escitalopram (Lexapro)
- Fluoxetine (Prozac)
- Paroxetine (Paxil)
- Sertraline (Zoloft)
- TCA (tricyclic antidepressants)
- Amitriptyline (Elavil)
Lifestyle Affects on Sleep Quality, the Sleep Architecture, and Restorative Sleep
A person's lifestyle choices can worsen restorative sleep. Alcohol prior to sleep and tobacco or nicotine usage can both negatively worsen the sleep architecture.
Alcohol is often used as a sleep aide. Alcohol does, indeed, shorten sleep latency or onset (or the period of time it takes for a person to fall asleep). However, alcohol disrupts sleep in four distinct ways:
- Alcohol causes you to sleep longer in the lighter sleep stages
- Alcohol causes you to briefly wake up (transient arousals) more frequently throughout the night (even though you won't remember waking up)
- Alcohol reduces cognitively-restorative Stage REM sleep
- Alcohol exacerbates underlying or pre-existing sleep disorders like sleep-disordered breathing, sleep apnea, snoring, and restless leg syndrome, which all then increase sleep architecture disruption, arousals, and further worsen restorative sleep even more than alcohol already does.
Tobacco is similar to alcohol in its effects on the sleep architecture. Nicotine withdrawal can begin to occur within a few hours after going to sleep, causing a person to experience elevated arousals (that they are unaware of) due to the body's cravings. Tobacco can also damage the upper airway, increasing the frequency of snoring or upper airway-related disturbances.
Improve your Sleep Architecture and Increase your Restorative Sleep to Relieve Fatigue and Improve Your Life
Improving your mood, energy, alertness, and overall quality of life begins with understanding the nature and severity of your sleep problem. We recommend sleep testing at an American Academy of Sleep Medicine (AASM) accredited sleep center or sleep lab like SleepSomatics. As the old adage goes, you can't get directions to your destination until you first determine where you are right now. Sleep is one-third of your life and therefore equally critical to your overall health regiment and medical care. You wouldn't trust a cancer diagnosis to a smart phone app; you'd demand credentialed, verified testing. The same logic holds for your sleep problem.
Getting older doesn't have to automatically mean weight gain, loss of energy, happiness, vitality, vigor, or satisfaction in your life and relationships. Sleep is the cornerstone of health, and restorative sleep deficiency can be the cause for your mental fatigue, anxiety, impotence, unhappiness, and weight gain. Screening for and treating sleep disorders is widely-available with most insurance plans. Sleep testing doesn't have to break the piggy bank! Your first step to improving the quality of your life is with an in-lab sleep study to evaluate and quantify the quality of your sleep at the Austin sleep lab SleepSomatics.
Concerned you aren't getting enough sleep? If you or someone you care about snores or is tired and fatigued during the day, sleep-disordered breathing (and sleep apnea) may be a serious risk. Get your sleep tested today by SleepSomatics, a professionally credentialed and accredited sleep test center located in Austin since 1999. Call 512.323.9253.
For more information, read this article's sources:
HuffPost Healthy Living: How Alcohol Can Ruin Your Sleep
Mayo Clinic: Monoamine oxidase inhibitors (MAOIs)
Medical News Today: What Are Benzodiazepines? What Are The Risks Of Benzodiazepines?
Medscape Critical Care: Effect of Medications on Sleep Onset and Architecture
Psychiatric Times: The Effects of Antidepressants on Sleep
This blog's thumbnail image credit goes to PsychCentral.